

Overview
Dermatophytosis, also known as ringworm, is a fungal skin infection, most often caused by one of three pathogens:
- Microsporum canis
- Microsporum gypseum
- Trichophyton mentagrophytes
All species have environmentally resistant fungal spores which can survive for months to years and it is a common zoonotic infection causing skin lesions in humans. Infection is caused by dermatophytes invade the hair follicle and shaft, although the disease may be self-limiting in healthy adult dogs. Clinical disease is more severe in young, elderly or immune-suppressed patients (including those receiving glucocorticoid therapy).
Transmission
Microsporum canis is transmitted by direct contact with infected animals (cats, dogs), fomites including grooming tools or shared environment. Yorkshire terrier dogs are more susceptible to ringworm infection than other breeds.
Trichophyton mentagrophytes predominates in wild animals, especially rodents, which act as a reservoir. Infection may be more common in dogs that hunt, with Jack Russel terriers being predisposed.
Microsporum gypseum is a geophilic dermatophyte found in the soil.
Clinical signs
Clinical signs are often variable, with some dogs being carriers and asymptomatic. Skin signs most often present as progressive patchy alopecia, most commonly affecting the head (particularly in dogs hunting rodents), pinnae, tail and limbs (Figure 1).


Pruritus is usually mild and common signs are scale, inflammation of skin and papule formation. Deep infections of the skin may result in folliculitis, furunculosis and scarring. Infection of nails produces distorted nails that can fracture and fall off.
Fungal kerion formation - these are focal immune-based inflammatory response to dermatophyte or fungal products. They can occur anywhere on body, most frequently on face, muzzle and paws and are more common in Boxer and Golden Retriever breeds of dog. They often appear as solitary raised skin lesion with alopecia and can have multiple punctuate draining tracts with erosion of overlying skin (Figure 2). Pruritus, self-trauma and secondary bacterial skin infection are common, with localised pain and local peripheral lymphadenopathy.

Diagnostic investigations
Wood's lamp examination of hairs (50% of hairs infected with Microsporum canis fluoresce green in ultraviolet light).
Microscopy of skin scrape mounted in 10% potassium hydroxide or lactophenol cotton blue to identify ectothrix arthroconidia spore.
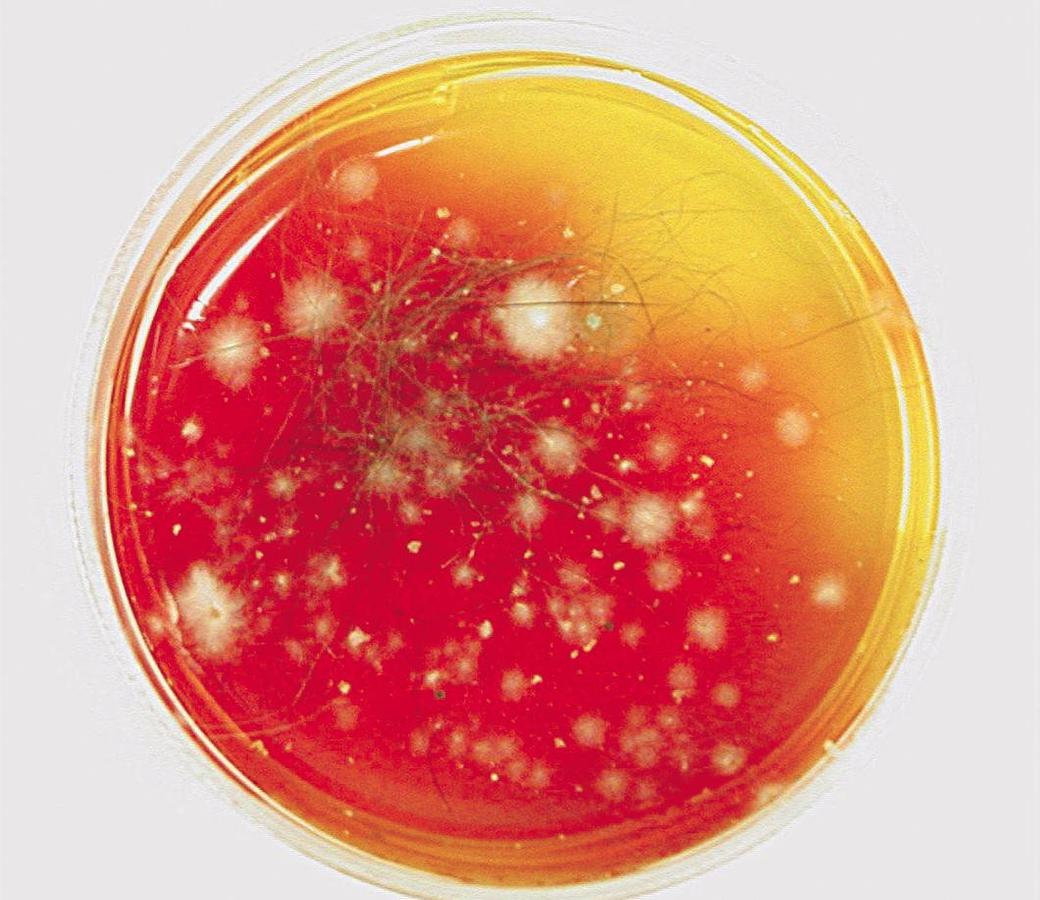
Dermatophyte culture of skin scrape, hair pluck or tooth brushing from affected area. This requires specific fungal culture medium (Dermatophyte Test Medium or Sabouraud's agar) and takes 14 days. A positive culture on DTM is identified by a red colour change within 7 days corresponding to early dermatophyte growth.
Fungal kerion - histology of nodule – special stains to identify fungal components required.
Treatment
Prolonged courses of treatment may be necessary and should be continued until mycological cure is obtained, constituting two negative cultures two weeks apart.
Anti-fungal shampoo:
- Chlorhexidine 2% + Miconazole 2% use to bathe dog 2–3 times weekly
- Lather and stand for 10 minutes before rinsing well
- Do not instil into ears (ototoxic). Do not use on or near eyes
Systemic medication:
- Itraconazole 5mg/kg or ketoconazole 5-10mg/kg orally with food every 24 hours. 4–20 weeks of treatment may be required depending on culture results. Treatment should be continued until mycological cure is obtained (see above)
- Contraindicated during pregnancy. Avoid in patients with hepatic disease
- May cause gastrointestinal side-effects – vomiting, diarrhoea, anorexia, salivation, abdominal pain. Also hepatotoxic, drug eruptions and ulcerative dermatitis, limb oedema
Topical leave-on products:
- Lime sulphur applied as a leave on spray, effective low cost treatment but stains and pungent smell
- Enilconazole applied as a leave on spray, effective well tolerated
Topical antifungal cream applied to discrete lesions:
- Clotrimazole 1% cream applied to affected area every 12 hours. If no improvement in 4 weeks, re-evaluate diagnosis and treatment
- Careful clipping and disposal of local hair
- Care should be taken to minimise risk of zoonosis when clipping the coat
Fungal kerion:
- Systemic anti-fungal treatment as above
- Antibiotic therapy for secondary bacterial infection:
- Amoxicillin/clavulanate 12.5mg/kg twice daily orally
- OR Cephalexin 25mg/kg twice daily orally
Remove of scale and dander from the environment and bedding by vacuuming and disinfection is critical to remove spores, along with disinfection of grooming tools. All in-contact pets should also be treated as potential asymptomatic carriers. Appropriate hygiene precautions to prevent zoonotic infection – gloves and protective clothing when handling affected and in contact animals and bedding.
Prognosis
In most cases clearance of infection is successful with appropriate treatment. Severe disease may be more difficult to treat and manage if underlying disease or immune incompetence exists.
Prevention
Isolation of affected patients to prevent spread and zoonosis. Cleaning and disinfection of the environment, bedding and fomites useful products include sodium hypochlorite (50:50 dilution) and enilconazole. Treatment of all in contact animals.
Links
Further information on this subject is available on the ESCCAP website.